A typical pitch for venture capital investment highlights three topics: the problem a technology solves, the size of the market, and the profit potential
of the product. But at the pitches I witnessed from innovators last Thursday at the Saving Lives at Birth DevelopmentXChange, this formula was turned on its head. While the discussion focused on problem solving,
the questions being asked were not how large the market, but how great the need, and not how much money can be made, but how many lives could be saved.
The DevelopmentXChange marked the final stage of competition in the 6th annual Saving Lives at Birth Grand Challenge,
a prize program sponsored by the US Agency of International Development, the government of Norway, the Bill & Melinda Gates Foundation, Grand Challenges
Canada, the UK Department of International Development, and the Korea International Cooperation Agency to identify and advance transformative, cost-effective
solutions to improve maternal and newborn health. The program operates much like a venture capital firm. Innovators apply and pitch their ideas, and
the program determines whether to issue them grants to develop, test, and bring their ideas to scale.
This year the program received more than 650 applications from 78 countries, with 49 teams chosen as finalists to compete at this year’s DevelopmentXChange and showcase their innovations. At the conclusion of
the event, Saving Lives at Birth announced the selection of 12 winning teams in the validation and seed grant categories, who will receive more than $3.4 million in funding to move their
projects forward. Award winners in the transition-to-scale category will be announced later this year.
GHTC members featured among finalists
Among the 48 finalists were five promising innovations from GHTC member organizations, profiled below:
Finalization and validation of a postpartum screening tool focused on identifying risk factors for maternal infection as part of routine, predischarge service delivery
Jhpiego
Despite widespread availability of treatment, postpartum infections account for 11 percent of maternal deaths worldwide. A number of risk factors are strongly associated with postpartum infection, and symptoms
usually manifest within 48 hours after birth. In Uganda, women are increasingly giving birth in hospitals; however, they are often discharged early
due to overcrowding.
To address this challenge, Jhpiego has developed a simple screening tool to assess a woman’s risk of postpartum infection. The tool is a checklist of the
key risk factors, composed of eight yes or no questions. The assessment is easy to use, and the results are even easier to interpret. If the tool proves
to be predictive of postpartum infection, it could be used by health workers, including nurses and midwives, to make evidence-based decisions on whether
a new mother can be safely discharged or whether she should remain in the hospital for an additional 48 hours. At Saving Lives at Birth, Jhpiego was
seeking funding to finalize and validate the tool—to determine its predictive value—by rolling it out in two regional referral hospitals
in Uganda. If successful, Jhpiego plans to partner with the ministry of health to expand its use across public- and private-sector hospitals.
Field validation of a new protein-to-creatinine (PrCr) strip test: An impactful new tool to improve diagnosis of preeclampsia at the front lines of antenatal care in low-resource settings
PATH
At least 16 percent of maternal mortality worldwide is attributable to preeclampsia, a dangerous condition that can cause organ failure, seizures, and
maternal and newborn death. Screening for preeclampsia—which is characterized by high blood pressure and protein in urine (proteinuria)—ideally
occurs as part of the care a woman receives during pregnancy. Throughout the day, the concentration of urine often fluctuates, and so, too, does the
concentration of protein in the urine. Consequently, the gold standard for diagnosing proteinuria involves collecting and analyzing urine samples over
24 hours. However, this approach is unrealistic in many low-resource settings, and current diagnosis involves a protein-only dipstick test that catches
just 51 to 68 percent of cases.
PATH has developed a simple, low-cost protein-to-creatinine strip test to improve the accuracy of preeclampsia screening in low-resource settings and was
seeking funding through the Saving Lives at Birth program to evaluate the feasibility and efficacy of the diagnostic test in Ghana. The test is nearly
identical to the commonly used protein-only test. However, where the existing tool only tests for protein concentration, the new device also tests
for creatinine concentration. By comparing the concentration of both protein and creatinine, a health worker can control for how diluted or concentrated
the urine is at the time. PATH has confirmed that the diagnostic strip remains effective when stored for at least four months at 37 to 45°C, and the
tool costs just pennies on the dollar. Due to its similarity to the existing protein-only test, rollout of the test should be straightforward, requiring
very little additional training.
Developing a Rapid Integrated Sepsis Risk Calculator (RISC) to detect and manage severe sepsis in newborns
PATH
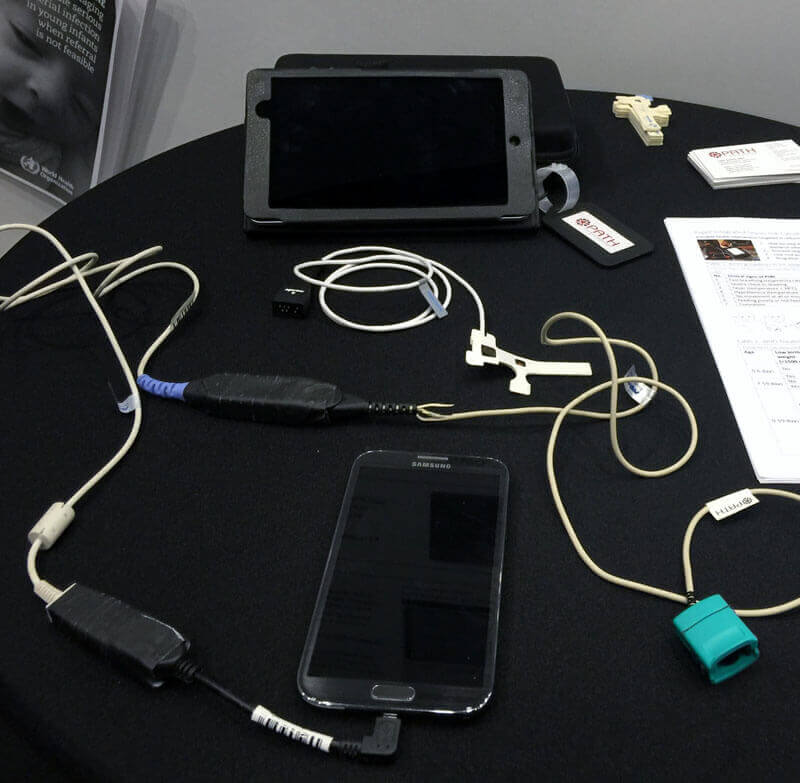 PATH's Rapid Integrated Sepsis Risk Calculator. Photo: Matthew Robinson/GHTC
PATH's Rapid Integrated Sepsis Risk Calculator. Photo: Matthew Robinson/GHTC
Sepsis kills an estimated 421,000 infants in the first 28 days of life in low- and middle-income countries every year. To address this glaring need, the
World Health Organization (WHO) recently published guidelines for diagnosis and treatment of possible serious bacterial infection (PSBI), which will
require primary-level health care providers to be versed in sepsis detection and management. Many providers do not currently have the necessary training
or tools.
The RISC is a smartphone or tablet-based app and off-the-shelf device measuring oxygen saturation levels in the blood that enables even primary-level providers
to identify sick infants and either provide the correct treatment or refer them to higher-level care. The app incorporates algorithms that walk the
provider step by step through the diagnostic process, increasing provider confidence and greatly improving the accuracy of diagnoses. Because the app
will be built using Open Data Kit (ODK) free open-source software and off-the-shelf hardware, it will be highly cost-effective and adaptable. The app
also works offline, which is critical in remote primary care facilities. The team was seeking a Saving Lives at Birth seed award to complete the development
of the ODK app and conduct a pilot evaluation of RISC’s usability, feasibility, and acceptability in Ghana.
Development and evaluation of the RELI Delivery System—an innovative, simplified, low-cost infusion pump for obstetric and newborn emergencies
PATH
With a few pumps of a handle, a health worker can power an intravenous fluid infusion pump for an entire work shift, all without the use of electricity
or batteries. That’s the idea behind PATH’s RELI Delivery System—an innovative, low-cost infusion pump for obstetric and newborn care.
Controlled intravenous delivery of medicines like antibiotics or anesthesia is the gold standard of care for many diseases and conditions, but it’s often
not feasible in low-resource settings. Existing infusion pumps cost thousands of dollars to purchase and maintain, require substantial training to
operate, and require electricity or batteries. PATH designed the RELI System to overcome many of these barriers to access in low-resource settings.
The device, which requires no electricity or batteries, is powered pneumatically, through air pressure. It requires about two minutes of pumping to
generate the power needed to operate the device for an entire 12-hour shift. The system also has a simple-to-use interface and can be manufactured
inexpensively, with an expected retail price at less than $100 a machine. With the seed grant it won through the program, PATH plans to take the device
to the field to solicit user feedback and then refine the design for further field testing.
Outpatient treatment of neonatal sepsis by rectal administration of gentamicin
PATH
Neonatal sepsis is a leading cause of infant death worldwide. WHO recommends treatment of the condition with intramuscular injection of the commonly used
antibiotic gentamicin. But in many low-resource settings, this is easier said than done. Neonatal dosing is extremely sensitive—just a fraction
of a difference in dose size can affect effectiveness and safety—so administration requires a highly trained health worker. Additionally, many
health providers may not have access to safe injection devices or may be inclined to reuse needles, promoting the spread of the disease.
Unfortunately, gentamicin is not effective when delivered orally, so PATH is exploring the feasibility of an alternative method of gentamicin delivery—rectal
delivery. As a needle-free method of administration, rectal delivery could improve access to gentamicin by making it safer for the product to be administered
by lower-level health workers, increasing dose accuracy, and removing the risks associated with injections. Existing scientific literature suggests
rectal delivery could be a biologically viable option for gentamicin. PATH was seeking a grant to conduct further lab studies to assess how different
additives or formulations can improve uptake of gentamicin in colon cells and conduct stakeholder interviews to assess feasibility of the concept.
The innovation effect
GHTC congratulates both our members and the other teams who were selected as finalists and award winners.
This year’s prize winners will join the growing community of over 93 innovators supported by the Saving Lives at Birth program. Many of these innovations
are beginning to have an impact as they are brought to scale. To date, the program has supported 1.5 million women and newborns and saved nearly 10,000
lives.
The Saving Lives at Birth program has made it clear that by putting innovation at the center of global health, we can accelerate the pace of change and
transform lives, faster.
Kat Kelley, senior program assistant, and Matthew Robinson, MA, policy officer, contributed to this article.